PADI IDC TAUCH-THEORIE
Tauchtheorie – Physiologie ist eines der 5 Themen, die bei der PADI Tauchlehrerprüfung geprüft werden.
Wir haben diese Materialien zur Verfügung gestellt, damit du dich auf die PADI Instructor Prüfung oder PADI Divemaster Prüfung
vorbereiten kannst.
Wenn du dich entscheidest, deinen PADI Divemaster Kurs oder PADI IDC mit Asia Scuba Instructors zu machen, wirst du Zugang zu vielen weiteren Materialien haben, in ‘online classroom’.
Physiologie

Das Herz-Kreislauf-System
Der menschliche Körper braucht Sauerstoff, um chemische Energie in nutzbare Lebensenergie umzuwandeln.
Das Atmungssystem bringt Sauerstoff in den Körper und transportiert Kohlendioxidabfälle aus dem Körper. Es transportiert auch Stickstoff zu den Körpergeweben und und führt es wieder weg. Der Blutkreislauf transportiert Kraftstoff, Materialien und Sauerstoff von den Atmungs- und Verdauungssystemen zum Körpergewebe und transportiert Abfallmaterial und Kohlendioxid wieder heraus.
Das Atmungssystem und der Blutkreislauf arbeiten zusammen und sind eng miteinander verbunden. Zusammen werden diese Systeme als -Kreislauf-System bezeichnet.
Der Blutkreislauf
Blut zirkuliert durch den Körper, um den Körper mit Sauerstoff zu versorgen. Das Blut besteht hauptsächlich aus Plasma, einer klaren Flüssigkeit, welche die Blutzellen trägt. Rote Blutkörperchen geben dem Blut eine rote Farbe. Die roten Blutkörperchen enthalten Hämoglobin, das sich mit Sauerstoff verbindet, damit dieser transportiert werden kann. Weiße Blutkörperchen bekämpfen Infektionen und die Blutplättchen (Thrombozyten) sind für die Blutgerinnung verantwortlich.
All dies wird vom Herzen durch den Körper gepumpt. Blutgefäße, die Blut vom Herzen wegführen, werden als Arterien bezeichnet. Blutgefäße, die Blut zum Herzen zurückführen, werden als Venen bezeichnet. Zwischen den Arterien und den Venen befinden sich kleine Blutgefäße, in denen das Gewebe Sauerstoff aufnimmt und CO2 freisetzt – diese werden als Kapillaren bezeichnet.
Der Körper reagiert auf das Eintauchen in kaltes Wasser, indem er die Herzfrequenz verlangsamt (Bradykardie). Dies wird auch als der Säugetier-Tauchreflex oder einfach der Tauchreflex bezeichnet. Aus diesem Grund können Ertrinkungsopfer in sehr kaltem Wasser manchmal wiederbelebt werden, selbst nachdem sie lange Zeit untergetaucht waren.
Der Karotissinus-Rezeptoren überwachen den Druck des arteriellen Blutes, das das Gehirn erreicht.
Die Rezeptoren interpretieren den Druck, der von einer zu engen Kapuze, der Halsmanschette eines Neoprenanzugs oder der Halsmanschette eines Trockenanzugs ausgeht, als hohen Blutdruck. Dies führt dazu, dass das Herz langsamer schlägt (Bradykardie), wodurch der Blutfluss zum Gehirn verringert wird. Der Taucher kann sich benommen fühlen, und wenn dies anhält, kann es zur Bewusstlosigkeit führen. Dies nennt man Karotis-Sinus-Reflex.
Das Einatmen kontaminierter Luft kann zu einer Kohlenmonoxidvergiftung führen. Hämoglobin verbindet sich 200-mal leichter mit Kohlenmonoxid als mit Sauerstoff. Wenn das passiert kann das Hämoglobin weniger Sauerstoff durch den Körper transportieren und der Taucher kann aufgrund von Sauerstoffmangel (Hypoxie) ohnmächtig werden. Anzeichen und Symptome sind Kopfschmerzen, Verwirrtheit, Sehstörungen, leuchtend rote Lippen und Fingernagelbetten.
Das Atmungssystem
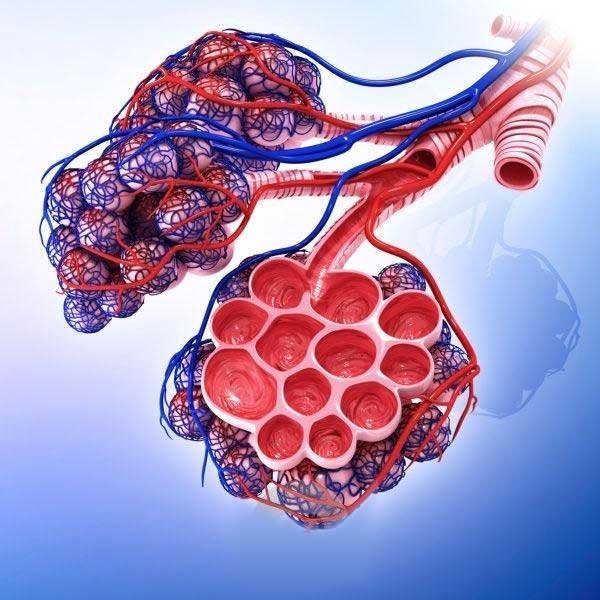
Die Luft strömt durch Mund und Nase ein und gelangt in den Trachea (Luftröhre) Die Luftröhre verzweigt sich in die rechte und linke Bronchien, die in die Lunge führen.
Die Lunge wird oft mit einem Ballon verglichen, ist aber eigentlich eher ein Schwamm.
Im Inneren der Lunge teilen sich die linken und rechten Bronchien in immer kleinere Bronchiolen bis zum Erreichen der Alveolen, kleine Säcke, die von den Lungenkapillaren umgeben sind. Hier findet der Gasaustausch statt.
Reaktionen auf das Tauchen
Für einen maximalen Gasaustausch muss langsam und tief geatmet werden. Wenn ausgeatmet wird, bleibt ein Teil der Luft in den Lungen und im Hals zurück. Diese Räume werden als Totraumvolumen bezeichnet. Die Luft aus dem Totraumvolumen (niedriger Sauerstoff- und hoher Kohlendioxidgehalt) wird beim nächsten Atemzug wieder mit eingeatmet. Schnorchel und Atemregler vergrößern das Totraumvolumen. Flaches, schnelles Atmen führt zur Akkumulation von Kohlendioxid, bekannt als Hyperkapnie, wodurch sich der Taucher außer Atem fühlt. Dies kann auch verursacht werden, wenn sich der Taucher überanstrengt oder auch durch einen schlecht gewarteten Atemregler, aus dem es sich schwer atmen lässt.
Der Atemreflex wird in erster Linie durch einen Überschuss an Kohlendioxid ausgelöst - nicht so sehr durch einen Mangel an Sauerstoff. Wenn ein Atemtaucher (Freediver) hyperventiliert, reduziert dies das CO2 in der Lunge und verlängert die Zeit, bevor der Taucher den Drang zu atmen verspürt.
Bei übermäßiger Hyperventilation wird der CO2-Gehalt in der Lunge zu stark reduziert (Hypokapnie), so dass der Sauerstoffgehalt unter Wasser unter einen kritischen Wert fällt, bevor das CO2 den Drang zum Atmen auslöst. Während sich der Taucher in der Tiefe befindet, ist der Sauerstoffpartialdruck in der Lunge hoch genug, damit ein Gasaustausch stattfinden kann (denke an die Physik). Wenn der Taucher aufsteigt, sinkt der Sauerstoffpartialdruck und der Taucher kann ohnmächtig werden aufgrund von Hypoxie (Sauerstoffmangel). Dies ist bekannt als Flachwasser-Blackout da dies oft kurz bevor der Freediver die Oberfläche erreicht, geschieht.
Beinahe-Ertrinken tritt dann auf, wenn eine Person im Wasser erstickt, aber wiederbelebt wird. Gib dem atmenden Patienten Notsauerstoff, halte den Patienten im Liegen und behandele ihn gegen Schock. Der Patient sollte medizinisch versorgt werden, auch wenn er sich vollständig erholt zu haben scheint. In die Lunge eingedrungenes Wasser kann physiologische Komplikationen verursachen, die die Fähigkeit der Lunge zum Gasaustausch beeinträchtigen. Dies kann zu sekundärem Ertrinkenführen, das lebensbedrohlich ist.

Stickstoff (Gas) Narkose:
Das Einatmen von zu viel Stickstoff kann zu einer narkotischen Wirkung führen (Stickstoffnarkose). Eine Narkose kann beim Tauchen auf 30 m oder tiefer auftreten, sie ist von Taucher zu Taucher unterschiedlich und nicht vorhersehbar. Zu den Symptomen können Euphorie (Glücksgefühl), Ängstlichkeit (Furcht), Panik, Schwindel, Tunnelblick gehören.
Symptome, die nicht direkt gefährlich sind - aber beeinträchtigtes Urteilsvermögen und Koordinationsverlust können zu einer gefährlichen Situation führen. Ein Auftauchen um einige Meter verringert normalerweise die Narkose. Das Tauchen mit angereicherter Luft - Nitrox - verringert das Risiko einer Stickstoffnarkose nicht, da auch Sauerstoff eine narkotisierende Wirkung haben kann.
Sauerstoff-Toxizität
Toxizität für das zentrale Nervensystem (ZNS) - wird durch das Einatmen von zu viel Sauerstoff verursacht. Sporttaucher riskieren eine ZNS-Toxizität, wenn sie Sauerstoff mit einem Partialdruck von mehr als 1,4 bar einatmen.
Das schwerwiegendste Symptom ist ein Krampfanfall, der dazu führen kann, dass der Taucher sein Mundstück verliert und ertrinkt. Weitere Anzeichen und Symptome sind: Sehstörungen, Ohrensausen, Übelkeit, Zuckungen, Reizbarkeit und Schwindel (VENTID). Krämpfe treten jedoch in der Regel ohne Vorwarnung auf.
Lungentoxizität - entsteht dadurch, dass die Lunge über einen längeren Zeitraum einem hohen Sauerstoffpartialdruck ausgesetzt ist.
Zu den Anzeichen und Symptomen gehören Brennen in der Brust und Reizhusten. Es ist sehr unwahrscheinlich, dass dies beim Sporttauchen vorkommt.
Dekompressionskrankheit
Gase lösen sich in Flüssigkeiten wenn der Druck auf die Flüssigkeit erhöht wird. Der menschliche Körper besteht hauptsächlich aus Flüssigkeit. Wenn ein Taucher unter Druck ein Gas atmet, löst sich dieses Gas im Körpergewebe. Sauerstoff wird vom Körper verwendet, Stickstoff (und jedes andere Inertgas) jedoch nicht. Wenn der Stickstoffdruck in der Lunge höher ist als im Blut, löst sich Stickstoff (in den Alveolen) im Blut und dann im Gewebe auf. Die Menge an Stickstoff, die der Körper aufnimmt, hängt von der Tiefe und der Länge des Tauchgangs ab. Es kommt auch auf das Atemgas an. (Mit Sauerstoff angereicherte Luft – Nitrox – enthält weniger Stickstoff).
Wenn der Taucher an die Oberfläche steigt, wird der Stickstoffdruck im Gewebe höher als der Umgebungsdruck. Der Stickstoffdruck im Blut übersteigt den Druck in der Lunge und Stickstoff löst sich aus dem Blut (in den Alveolen) in der Lunge auf und wird ausgeatmet. Wenn der Unterschied gering ist, löst sich Stickstoff harmlos aus dem Blut heraus und tritt dann langsam durch Ausatmen aus. Wenn der Körper zu viel Stickstoff aufgenommen hat, kann der Körper den Stickstoff nicht so schnell eliminieren (ausatmen), wie er aus der Lösung austritt, und es können sich Blasen im Blut und im Gewebe bilden. Stickstoffblasen können die Sauerstoffzufuhr zum Körpergewebe blockieren. Dies ist als Dekompressionskrankheit bekannt.
Es kommt häufig vor, dass Taucher nach einem Tauchgang mikroskopisch kleine Stickstoffblasen in ihrem Körper haben. Diese harmlosen Bläschen sind bekannt als stille Blasen. Nach einiger Zeit, und wenn während des Tauchgangs zu viel Stickstoff aufgenommen wurde, können sich diese stillen Blasen nach und nach ansammeln und größere Blasen bilden.

Anzeichen und Symptome
Anzeichen und Symptome einer Dekompressionskrankheit treten tendenziell verspätet auf. In etwa der Hälfte der Fälle tritt es innerhalb einer Stunde auf, es kann jedoch bis zu auch 36 Stunden dauern, bis Anzeichen und Symptome auftreten. In den ersten Stunden verschlechtern sich diese oft.
Es gibt zwei Arten von DCS, abhängig von den Anzeichen und Symptomen und dem Schweregrad.
Typ I– (nur Schmerzen) ist nicht sofort lebensbedrohlich und es ist unwahrscheinlich, daß es zu einer langfristigen Behinderung kommt. Dies zeigt sich durch einen Hautausschlag, häufig in Körperteilen mit viel Fettgewebe.
Typ II – wirkt sich auf das Nervensystem aus und kann sofort lebensbedrohlich sein. Anzeichen und Symptome sind Kribbeln, Taubheitsgefühl, Lähmungen, schlaganfallähnliche Symptome, Bewusstlosigkeit und Herz- oder Atemstillstand. Wenn Blasen zum Gehirn wandern, können Anzeichen und Symptome verschwommenes Sehen, Verwirrung, Kopfschmerzen, Bewusstlosigkeit und Tod sein.
Prädisponierende Faktoren
Da jeder Mensch eine andere Physiologie hat, ist die Prädisposition für DCS von Person zu Person unterschiedlich. Faktoren, die einen Taucher für DCS prädisponieren können:
Fettgewebe -Stickstoff ist besser in Fett löslich.
Alter -Die Kreislaufsysteme werden weniger effizient; ein erhöhter Fettanteil und ein geringeres Fitnessniveau könnten die Stickstoffausscheidung verringern.
Dehydrierung -Die verringerte Blutmenge im Kreislauf verlangsamt die Stickstoffausscheidung.
Verletzungen oder Krankheiten -Verletzungen oder Krankheiten können die Effizienz des Kreislaufsystems beeinträchtigen.
Alkohol -Das Trinken von Alkohol vor oder nach (!) dem Tauchen beschleunigt die Durchblutung, erweitert die Kapillaren und fördert die Dehydration.
Kaltes Wasser -Ein Taucher beginnt einen Tauchgang warm und mit normalem Kreislauf, kühlt aber ab und die Durchblutung der Extremitäten wird reduziert, was die Stickstoffausscheidung verlangsamt.
Schweres Training - Wenn man sich während eines Tauchgangs anstrengt, beschleunigt sich der Kreislauf, so dass sich mehr Stickstoff als normal im Körper auflöst. Nach oder unmittelbar vor einem Tauchgang beschleunigt schwere körperliche Betätigung den Kreislauf, wodurch sich die Stickstoffausscheidung verändert und die Produktion von Mikrobläschen angeregt wird.
Höhenlage oder Fliegen nach dem Tauchen -Tauchtabellen und Computer basieren auf dem Auftauchen auf Meereshöhe. Ein niedrigerer Druck erhöht den Druckgradienten im Gewebe und kann die Blasenbildung verstärken.
Vorgeschichte einer Dekompressionskrankheit -Studien über Taucher legen nahe, dass jemand, der schon einmal an DCS erkrankt war, in Zukunft eher dazu neigt.
Patent Foramen Ovale (PFO)
Ein PFO, allgemein als "Loch im Herzen" bekannt, ist eine Öffnung im Herzen (vom rechten zum linken Vorhof), die sich normalerweise nach der Geburt verschließt. Bei etwa 30% der normalen und gesunden Bevölkerung wächst das PFO jedoch nicht vollständig zu.
Ein PFO erhöht das Risiko einer Dekompressionserkrankung, da Blasen direkt aus dem venösen Blut (sauerstoffarmes Blut, das zum Herzen zurückfließt) in den arteriellen Kreislauf gelangen können, der den Sauerstoff zum Gewebe transportiert.

Behandlung von DCS
Behandle alle Fälle ernst. Gib dem Patienten Sauerstoff, vorzugsweise 100 Prozent. Halte den Patienten mit gestütztem Kopf im Liegen. Überwache den Patienten und arrangiere den Transport zur nächsten medizinischen Einrichtung.
Lungenüberdehnungen
Dies kann passieren, wenn ein Taucher den Atem anhält, während er an die Oberfläche steigt. Durch den verringerten Druck steigt das Lungenvolumen an. Dies kann zu einem Riss in der Lunge führen, durch den Luft entweichen kann – daher der Begriff „Lungenriss“. Tauchen mit einer Lungenentzündung erhöht das Risiko einer Lungenüberdehnung, ebenso wie das Rauchen.
Es gibt vier Arten von Verletzungen, die auftreten können:
Luftembolie: Die Luftembolie ist die schwerwiegendste Verletzung unter den Lungenüberdehnungen. Hierbei gelangt Luft durch gerissene Alveolen in die Lungenkapillaren und anschließend in den Blutkreislauf. Die Luftblasen können stecken bleiben und den Blutfluss behindern. Dies ist lebensbedrohlich, da die Blasen durch die Arterien zum Gehirn fließen können.
Pneumothorax: (Lungenkollaps). Beim Pneumothorax reißt die Lunge an der Oberfläche. Luft dringt zwischen Lunge und Rippenfell. Die Folge ist, daß die Lunge teils oder ganz in sich zusammenfällt. Der Patient hat starke Brustschmerzen und Atemnot.
Mediastinales Emphysem: Beim Mediastinalemphysem sammelt sich Luft zwischen den Lungenflügeln an. Die angesammelte Luft kann auf das Herz und die Hauptblutgefäße drücken und so die Zirkulation beeinträchtigen. Anzeichen sind Luftnot und Bewusstlosigkeit.
Subkutanes Emphysem: Die Luft sammelt sich direkt unter der Haut im Nacken- und Schulterbereich an. Der Taucher bemerkt eine Klangveränderung seiner Stimme. Meist knistert die Luft unter der Haut bei Berührung.
Dekompressionserkrankung
Eine Dekompressionskrankheit wird verursacht durch Stickstoffblasen die aus der Lösung austreten. (Auf Englisch decompression sickness – DCS) Bei einer Lungenüberdehnung kommen Luftblasen durch eine gerissene Lunge in das Körpergewebe. Die Dekompressionserkrankung (Auf Englisch decompression illness – DCI) deckt die Dekompressionskrankheit und alle Typen der Lungenüberdehnungen ab.
Die Anzeichen und Symptome für eine Dekompressionskrankheit und Lungenüberdehnungsverletzungen sind sehr ähnlich. Bei einer Lungenüberdehnung treten die Anzeichen und Symptome normalerweise direkt nach dem Tauchgang auf, während es bei der Dekompressionskrankheit mehrere Stunden oder sogar Tage vergehen können.

Überhitzung
Überhitzung (Hyperthermie) ist ein potenzielles Problem für Taucher, die an einem heißen Tag einen langen Neoprenanzug tragen. Der Körper reagiert auf überschüssige Wärme, indem er zuerst die Hautkapillaren erweitert, um die Kühlung zu fördern. Wenn dies nicht hilft, kühlt Schwitzen die Haut ab. Als nächstes wird der Puls erhöht, um das Blut zum Abkühlen schneller zirkulieren zu lassen.
tritt auf, wenn der Körper mit voller Kühlleistung arbeitet. Anzeichen und Symptome sind ein schwacher und schneller Puls, starker Schweiß, kühle und feuchte Haut, Übelkeit und Schwäche. Diese Person muss sich abkühlen. Also den Anzug ausziehen oder im Wasser abkühlen.
Ein Hitzschlag entsteht, wenn der Körper an seine Grenzen stößt und sich nicht weiter abkühlen läßt. Das Schwitzen hört auf, die Haut ist heiß und gerötet und der Puls ist kräftig aber dennoch schnell. Dies ist eine medizinische Notsituation, die das Gehirn und das Körpersystem ernsthaft schädigen kann.
Unterkühlung
Wasser leitet Wärme 20-mal schneller ab als Luft. Deshalb werden wir auch in relativ warmem Wasser abkühlen.
Wenn der Körper Wärme verliert, reagiert er, indem er den Blutfluss zu den Extremitäten verringert (Finger und Zehen werden taub). Wenn der Körper zu zittern beginnt, um durch Muskelaktivität Wärme zu erzeugen, ist dies ein Signal dafür, daß der Körper den Kampf gegen die Kälte verliert. Der Tauchgang sollte beendet werden
Unkontrollierbares Zittern geht einer Hypothermie voraus. Dies tritt auf wenn alle Schutzmaßnahmen fehlschlagen, das Zittern aufhört und der Taucher sich warm fühlt- die Körpertemperatur jedoch weiter sinkt. Mentale Prozesse verlangsamen sich und der Taucher wird schläfrig, unkoordiniert und vergesslich. Hypothermie ist ein Notfall, der medizinische Versorgung erfordert.

Das Ohr
Das Ohr ist unterteilt in das Außen-, Mittel- und Innenohr.
Das Außenohr besteht aus Ohrmuschel und Gehörgang, ist offen für Luft- und Wasserdruck und leitet Schall zum Trommelfell. Das Mittelohr ist durch das Trommelfell vom Außenohr getrennt und von Luft und Wasser abgedichtet. Das Trommelfell vibriert und leitet den Schall an die Gehörknöchelchen weiter, die den Schall zum Innenohr leiten. Das Mittelohr ist mit Luft gefüllt und am stärksten vom Druck betroffen. Das Innenohr besteht aus den Bogengängen, die das Gleichgewicht steuern, und der Hörschnecke (Cochlea), die Vibrationen in Nervenimpulse umwandelt, die an das Gehirn gesendet werden.
Die Gehörknöchelchen verbinden sich mit der Hörschnecke durch das ovale Fenster, das sich mit den Vibrationen hinein und heraus bewegt. Das runde Fenster an der Cochlea wird herausgedrückt, wenn das ovale Fenster sich nach innen bewegt – wie ein wassergefüllter Ballon.
Das Mittelohr ist durch die Eustachische Röhre mit dem Hals und der Nase verbunden.
Druckverletzungen (Barotrauma) können während des Auf- oder Abstiegs auftreten. Wenn du die Struktur und Funktion von Ohren und Nebenhöhlen kennst, kannst du besser verstehen, wie sie durch Druckänderungen beeinflusst werden.
Druckprobleme beim Aufstieg werden als Umkehrblockierung bezeichnet. Während des Aufstiegs tritt expandierende Luft normalerweise leicht aus, wenn aber eine Blockierung das Austreten der Luft verhindert, kann eine Umkehrblockierung in Ohren und Nebenhöhlen auftreten.
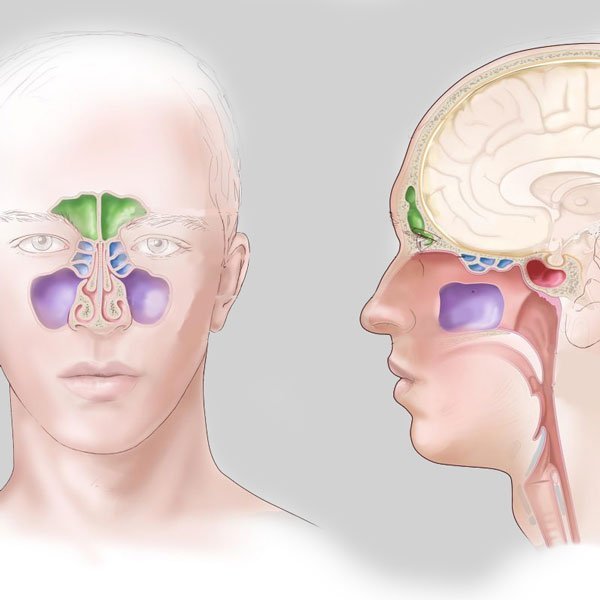
Nebenhöhlen
Die Nebenhöhlen sind in vier Kammern unterteilt und mit der Nase verbunden. Druckprobleme in der Nebenhöhlen verursachen Druckgefühle oder Schmerzen zwischen den Augen, über den Zähnen oder in den Wangenknochen. Blut und Flüssigkeit füllen die Hohlräume, um das Druckgleichgewicht wiederherzustellen. Während des Aufstiegs fließen angesammelte Flüssigkeiten und Blut häufig in die Tauchermaske. Die Nebenhöhlen heilen normalerweise von selbst. Es sei denn, es treten länger andauernde Schmerzen oder Fieber auf, was auf einen Infektion deutet.
Ohrenprobleme
Während des Abstiegs füllt Wasser das Außenohr und übt Druck auf das Trommelfell aus. Der Druck kann ausgeglichen werden, indem Luft durch die Eustachische Röhre in das Mittelohr gedrückt wird. Die meisten Taucher blasen gegen ihre eingeklemmte Nase – bekannt als Valsalva-Manöver. Wenn der Ausgleich nicht erfolgt, kann dies anschliessend zu einem Barotrauma führen.
Ein Barotrauma im führt dazu, daß Blut und Flüssigkeit das Mittelohr füllen. Die Ohren fühlen sich voll an und das Gehör ist eingeschränkt. Diese Verletzung muss zur Heilung ärztlich behandelt werden denn sie kann zu einem dauerhaften Hörverlust führen.
Ein Trommelfellriss kann auftreten, wenn ein Taucher ohne Druckausgleich schnell absteigt. Das Trommelfell biegt sich nach innen, bis es reißt und Wasser in das Mittelohr gelangt. Der Taucher wird einen scharfen Schmerz spüren, gefolgt von einer Erleichterung. Kaltes Wasser, das in das Mittelohr eindringt, kann Schwindel verursachen. Ein gerissenes Trommelfell erfordert ärztliche Hilfe, um Infektionen und dauerhafte Schäden zu vermeiden.
Ein weiteres Barotrauma des Ohrs ist ein Riss des runden Fensters. Wenn ein Taucher den Ausgleich verzögert, wölbt sich das runde Fenster als Reaktion auf ungleichen Druck nach außen. Wenn der Taucher nun gleichzeitig ein langes, kraftvolles Valsalva-Manöver versucht, kann der erhöhte Innendruck das runde Fenster reißen. Ein runder Fensterriss muss medizinisch behandelt werden und ist eine schwere Verletzung, die zu einer dauerhaften Hörminderung oder Taubheit führen kann .