PADI Dive Theory
PADI Dive Theory – Physiology is one of 5 subjects that will be tested on the PADI Instructor exam.
I have made these materials to help you to prepare for your PADI Instructor exam or PADI Divemaster exam. If you choose to do your PADI Divemaster course or PADI IDC with Asia Scuba Instructors you will have access to many more materials in our ‘online classroom’.
The PADI Dive Theory – Physiology Studyguide and practice exams are also available in German language.
Physiology

Cardiovascular system
The human body needs oxygen to convert chemical energy into usable energy for life.
The respiratory system brings oxygen into the body and carries waste carbon dioxide out of the body. It also carries nitrogen to and from the body.
The circulatory system transports fuel, materials and oxygen from the respiratory and digestive systems to the body tissues, and carries waste material and carbon dioxide from the tissues for elimination.
The respiratory and circulatory systems work together and are closely interlinked. Together these systems are referred to as the cardiovascular system.
Circulatory system
Blood circulates around your body to fuel the body with oxygen. The blood is made mainly of plasma, a clear fluidthat carries the blood cells.
Red blood cells give the blood a red color. The red blood cells contain haemoglobin which bonds with oxygen so that it can be transported.
White blood cells fight off infection and platelets help the blood to clot in case of injury.
All this is pumped around by the heart. Blood vessels carrying blood away from the heart are called arteries.
Blood vessels carrying blood back to the heart are called veins.
In between the arteries and veins are small blood vessels where the tissues take on oxygen and release CO2 – these are called capillaries.
Respiratory system
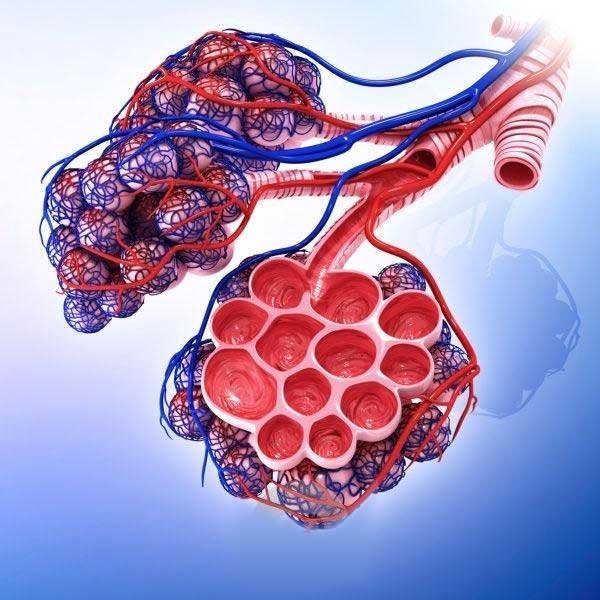
The air enters through the mouth and nose and enters the trachea (windpipe) The trachea branches into the right and left bronchi, which lead into the lungs.
The lungs are often compared with balloons but are actually more like sponges.
Inside the lungs, the left and right bronchi split into smaller and smaller bronchioles until reaching the alveoli; small sacs surrounded by the pulmonary capillaries. This is where the gas exchange takes place.
Responses to diving
For maximum gas exchange you need to breathe slow and deep. When you exhale, some of the air remains in your lungs and throat. These spaces are known as dead air spaces. The air from the dead air spaces (low oxygen- and high carbon dioxide level) is re-inhaled on the next breath. Snorkels and regulators make dead air space larger.
Shallow, rapid breathing causes a build-up of carbon dioxide, known as hypercapnia, which makes the diver feel out of breath. This can also be caused by the diver overexerting himself or a badly maintained regulator which is difficult to breathe from.
The breathing reflex is primarily triggered by an excess of carbon dioxide – not so much by a lack of oxygen. If a breath-hold diver hyperventilates, this reduces the CO2 in the lungs and extends the time before the diver gets the urge to breathe.
Excessive hyperventilation reduces the CO2 levels in the lungs too much (hypocapnia), so that when the diver is underwater the oxygen level drops below critical levels before the CO2 creates the urge to breath. While the diver is at depth, the partial pressure of the oxygen in the lungs is high enough for gas exchange to take place (remember the physics). When the diver ascends, the partial pressure of the oxygen drops and the diver can black out due to hypoxia (lack of oxygen). This is known as shallow water blackout as it often happens just before the breath-hold diver reaches the surface.
Near drowning occurs when a person suffers suffocation in water but is revived. Give the breathing patient emergency oxygen, keep patient lying down and treat for shock. The patient should seek medical care even when he or she seems fully recovered.
Water that has entered the lungs can cause physiological complications that interfere with the lung’s ability to exchange gases.
This can lead to secondary drowning, which is fatal.

Nitrogen (gas) Narcosis:
Breathing too much nitrogen can cause a narcotic effect (nitrogen narcosis). Narcosis can occur when diving to 30m or deeper, it varies from one diver to the next and is not predictable. Symptoms can include euphoria (feeling happy), anxiousness (fear), panic, dizziness, tunnel vision.
Symptoms which are not directly hazardous – but impaired judgment and loss of co-ordination can lead to a hazardous situation. Ascending a few meters usually reduces the narcosis. Diving with enriched air – Nitrox, does not reduce the risk of nitrogen narcosis because oxygen can also have a narcotic effect.
Oxygen Toxicity
Central nervous system (CNS) toxicity – is caused by breathing too much oxygen. Recreational divers risk CNS toxicity when breathing oxygen at partial pressures greater than 1.4 bar.
The most serious symptom is a convulsion which can cause the diver to lose his mouthpiece and drown. Other signs and symptoms include: visual disturbances, ear ringing, nausea, twitching, irritability and dizziness (VENTID). However, convulsions typically occur without warning.
Pulmonary toxicity – caused by exposing the lungs to high partial pressures of oxygen over a longer period.
Signs and symptoms include burning in the chest and an irritated cough. It is unlikely in recreational diving.
Decompression Sickness
Gases dissolve into liquids when the pressure on the liquid is increased.
The human body is primarily water. When a diver breathes gas under pressure, gases dissolve into the body tissues.
Oxygen used by the body, but nitrogen (and any other inert gas) is not.
When the nitrogen pressure in the lungs is greater than in blood, nitrogen (in the alveoli) dissolves into blood and then into the tissues.
The amount of nitrogen that the body absorbs depends on the depth and the length of the dive. It also depends on the breathing gas. (Enriched air has less nitrogen).
Wenn the diver ascends to the surface, nitrogen pressure in tissues becomes higher than the surrounding pressure.
The nitrogen pressure in the blood exceeds pressure in lungs and nitrogen dissolves from blood into the alveoli in the lungs and is exhaled.
If the difference is within limits, nitrogen dissolves harmlessly into blood and then slowly out through exhalations
If body has absorbed too much nitrogen, the body can not eliminate (breath out) as fast as it comes out of solution and bubbles form in the blood and tissues.
nitrogen bubbles can block the oxygen delivery to the body tissues. This is known as decompression sickness.
It is very common for divers to have microscopically small nitrogen bubbles in their body, after a dive. These harmless bubbles are known as silent bubbles. After time, and again, if too much nitrogen has been absorbed during the dive, these silent bubbles can accumalate to form larger bubbles.

DCS signs and symptoms
DCS signs and sympoms tend to be delayed. In about half the cases, it appears within an hour but it can take up to 36 hours for signs and symptoms to occur. It often worsens during the first few hours.
There are two types of DCS, depending on the signs and symptoms and severity.
Type I DCS– (pain-only DCS) is not immediately life-threatening or likely to cause long-term disability. This results in a skin rash, often in parts of the body that have a lot of fat tissue.
Type II DCS affects the nervous system and may be immediately life-threatening.
Signs and symptoms include tingling, numbness, paralysis, stroke-like symptoms, unconsciousness and cardiac or respiratory arrest. When bubbles travel to the brain, signs and symptoms can include blurred vision, confusion, headache, unconsciousness and death.
Predisposing factors
Because everyone has a different physiology, the predisposition to DCS varies from person to person. Factors that may predispose a diver to DCS:
Fat tissue –Nitrogen is more soluble in fat.
Age –Circulatory systems become less efficient; increased percentage of fat and reduced fitness level could decrease nitrogen elimination.
Dehydration –Reduced quantity of blood in circulation slows nitrogen elimination.
Injuries or illness –Injuries or illness can affect the efficiency of the circulatory system.
Alcohol –Drinking alcohol before or after diving accelerates circulation, dilates capillaries and promotes dehydration.
Cold water –A diver starts a dive warm with normal circulation, but cools and circulation to the extremities is reduced, slowing nitrogen elimination.
Heavy exercise – Working hard during a dive accelerates circulation thus more nitrogen than normal dissolves into the body. After or immediately before a dive, heavy exercise accelerates circulation, altering nitrogen elimination and stimulating the production of microbubbles.
Altitude or flying after diving –Dive tables and computers are based on surfacing at sea level –exposure to lower pressure increases tissue pressure gradient and may increase bubble formation.
History of DCS –Studies of divers suggest that someone who has had DCS will be more predisposed to it in the future.
Patent Foramen Ovale (PFO)
A PFO, commonly known as ‘hole in the heart’ is an opening in the heart (from the right atrium to the left atrium) that normally grows close after birth. In about 30% of the normal and healthy population, however the PFO does not grow completely closed.
A PFO increases the risk of decompression illness because bubbles may pass directly from the venous blood (oxygen poor blood, returning to the heart), into the arterial circulation that carries oxygen to the tissues.

Treatment for DCS
Treat all cases serious. Give the patient oxygen, preferably 100 percent. Keep the patient lying down with the head supported. Provide primary care and arrange transport to the nearest medical facility.
Lung over expansion injuries
This can happen when a scuba diver holds his breath while ascending to the surface. The reduced pressure causes the lung volume to increase. This can cause a tear in the lungs through which air can escape – hence, the term ‘ruptured lung’. Scuba diving with a lung congestion increases the risk of a lung over expansion injury, and so does loss of surfactant (fluid protecting the lung surface) due to smoking.
There are four types of injury that can occur:
Air embolism: This is also called arterial gas embolism (AGE). The alveoli and pulmonary capillaries rupture allowing air to directly enter the bloodstream and flow into the arteries. This is serious and immediately life threatening, because the bubbles flow through the arteries to the brain.
Pneumothorax: The air from the rupture goes between the lung and chest wall, causing the lung to collapse. The diver will have chest pain and may cough up blood.
Mediastinal emphysema: The air from the rupture accumulates in the centre of the chest over the heart and interferes with circulation; the diver may feel faint and short of breath.
Subcutaneous emphysema: The air from the rupture accumulates in the soft tissues under the skin, at the base of the neck. The diver’s voice may change and the skin may crackle to the touch.
Decompression illnes
Decompression sickness is caused by nitrogen bubbles coming out of solution.
A lung overexpansion injury is caused by air bubbles entering the body tissues through a ruptured lung.
DCI stands for decompression illness and covers DCS and all lung-overexpansion injuries.
The signs and symptoms for decompression sickness and lung overexpansion injuries are very similar, however, for a lung overexpansion the signs and symptoms normally occur directly after the dive while for decompression sickness it can take several hours or even days.

Responses to heat
Overheating (hyperthermia) is a potential problem for divers when fully suited on a hot day.
The body responds to excess heat progressively by first dilating the skin capillaries to promote cooling. If this doesn’t help, sweating starts to cool skin through evaporation
Next step is to accelerate the pulse to circulate blood faster for cooling.
Heat exhaustion occurs when the body works at full capacity to cool.
Signs and symptoms are a weak and rapid pulse, profuse perspiration, cool and clammy skin, nausea and weakness.
This person needs to cool off. Remove heavy exposure suit or cool in the water.
Heat stroke results if the body reaches its limits and fails to cool.
The sweating stops, person’s skin is hot and flushed, and pulse is strong but rapid.
This is an emergency medical condition that can cause serious damage to the brain and body systems.
Responses to cold
Water conducts heat 20 times faster than air, which is why we chill faster in even relatively warm water.
As the body loses heat, it responds by reducing blood flow to the extremities (fingers and toes go numb).
If the body starts shivering to generate heat through muscle activity, it is a signal that your body is losing the battle against cold. The correct reaction is to end the dive.
Uncontrollable shivering precedes hypothermia. This occurs when all protective responses fail, shivering stops and the diver feels warm, but core temperature continues to drop.
Mental processes slow and the diver becomes drowsy, uncoordinated and forgetful.
Advanced hypothermia is a medical emergency requiring emergency care.

The Ear
The ear is divided into the outer, middle and inner ear.
The outer ear consists of the external ear and ear canal, it is open to air/water pressure and channels sound to the eardrum.
The middle ear is separated from the outer ear by the ear drum and is sealed against air/water. The ear drum vibrates and passes sound to the ossicles, small bones that conduct sound to the inner ear. The middle ear is filled with air and is affected the most by pressure.
The inner ear consists of the vestibular canals that control balance and the cochlea which turns vibrations into nerve impulses that are sent to the brain.
The ossicles connect to the cochlea at the oval window which flexes in and out with the vibrations. The round window on the cochlea flexes out when the oval window flexes in, like a water filled balloon.
The middle ear is connected to the throat by the Eustachian tube .
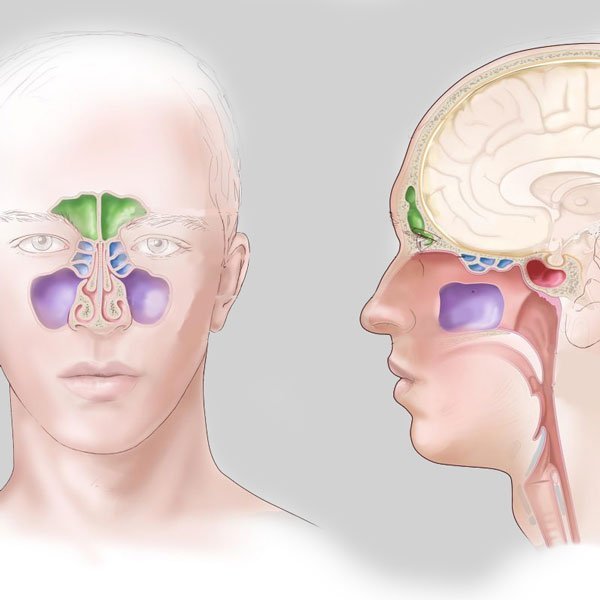
Sinuses
Sinuses are divided into four chambers and are connected to the nose.
A sinus squeeze causes pressure or pain between the eyes, over the teeth or in the cheekbones. Blood and fluid fill the sinus to restore pressure balance.
During ascent, accumulated fluids and blood often flow into the diver’s mask
A sinus squeeze usually heals on its own, unless accompanied by extended pain or fever, suggesting a sinus infection.
Ear trauma
During descent, water fills outer ear, putting pressure on eardrum.
The pressure can be equalized by pushing air through eustachian tubes into the middle ear.
Most divers blow against their pinched nose – known as the valsalva maneuver. Failure to equalize can cause a squeeze.
A middle ear squeeze results in blood and fluid filling the middle ear.
The ears feel full and hearing is reduced.
This injury needs proper treatment to heal because failure to receive medical care can mean permanent hearing loss.
An eardrum rupture can occur when a diver descends rapidly without equalizing. The eardrum flexes inward until it ruptures and water enters the middle ear. The diver will feel a sharp pain, followed by relieve. Cold water entering the middle ear can cause vertigo.
A ruptured eardrum requires medical attention to prevent infection and permanent damage.
Another ear barotrauma is round window rupture.
If a diver delays equalization, the round window bulges outward in response to unequal pressure. If at the same time, the diver attempts a long, forceful valsalva maneuver, the increased internal pressure can rupture the round window.
A round window rupture needs medical treatment and is a serious injury that can lead to permanent hearing reduction or deafness.